|
|
Septic Pulmonary Emboli
General Considerations
- Age
- Predisposed
- IV drug abusers
- Alcoholism
- Immunodeficiency
- CHD
- Dermal infection (cellulitis, carbuncles)
- Sources
- Tricuspid valve endocarditis
- Most common cause in IV drug abusers
- Pelvic thrombophlebitis
- Infected venous catheter or pacemaker wire
- Arteriovenous shunts for hemodialysis
- Drug abuse producing septic thrombophlebitis (eg, heroin addicts)
- Peritonsillar abscess
- Osteomyelitis
- Organism
Clinical Findings
- Sepsis
- Cough
- Dyspnea
- Hemoptysis
- Chest pain
- Shaking chills
- High fever
- Severe sinus tachycardia
- Location
- Predilection for lung bases
Imaging Findings
- Multiple round or wedge-shaped densities
- Cavitation
- Frequent
- Usually thin-walled
- Migratory
- Old ones clear and new ones arise
- Pleural effusion is rare
- Hilar and mediastinal adenopathy can occur
- CT findings
- Multiple peripheral parenchymal nodules
- Cavitation or air bronchogram in more than 89%
- Cavities are thin-walled and may have no fluid level
- Wedge-shaped subpleural lesion with apex of lesion directed toward pulmonary hilum (50%)
- Feeding vessel sign = pulmonary artery leading to nodule (67%)
Differential Diagnosis of Small Cavitary Lung Lesions |
Septic emboli |
Rheumatoid nodules |
Squamous or transitional cell metastases |
Necrotizing Granulomatosis |
Complications


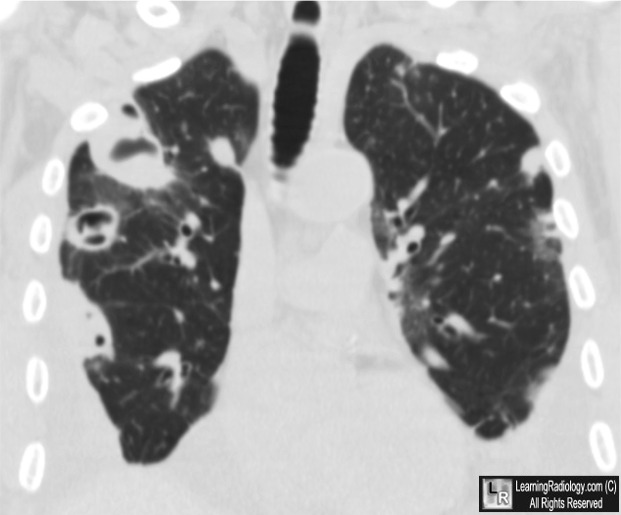
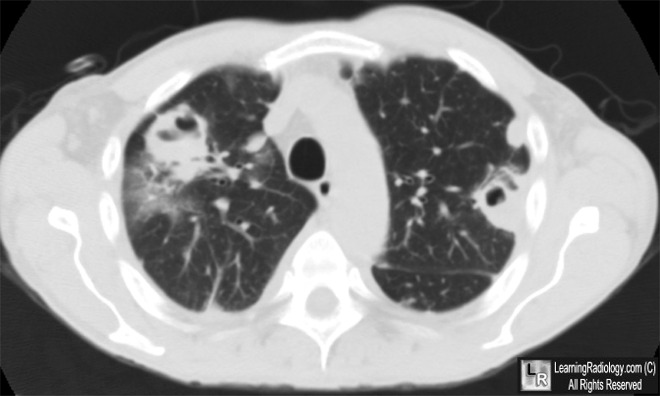
Septic Emboli. Upper photo. Coronal-reformatted CT of the chest shows multiple peripheral masses, most with cavitation (white arrows). Lower photo: Axial CT of chest demonstrates thin-walled upper lobe cavities.(white arrows). The patient was an intravenous drug user who was shown to have tricuspid vegetations by echo.
For these same photos without the arrows, click here and here
For more information, click on the link if you see this icon 
|
|
|

{kind=link}
{kind=link}